Gutter Boy
Tim Sherwood
COVID has created a whole industry of experts on subjects from hospital admissions, vaccine efficacy to "nudge theory." What will all these people do when the pandemic is over.
VAR and xG?
COVID has created a whole industry of experts on subjects from hospital admissions, vaccine efficacy to "nudge theory." What will all these people do when the pandemic is over.
COVID has created a whole industry of experts on subjects from hospital admissions, vaccine efficacy to "nudge theory." What will all these people do when the pandemic is over.
COVID has created a whole industry of experts on subjects from hospital admissions, vaccine efficacy to "nudge theory." What will all these people do when the pandemic is over.
COVID has created a whole industry of experts on subjects from hospital admissions, vaccine efficacy to "nudge theory." What will all these people do when the pandemic is over.
Not sure how sharing academical studies or discussing academical research makes anyone an expert. For example, if people are saying "I think Omicron is mild" then you'd be correct. If they're saying "I read a research paper highlighting lower impact on lung replication" then that doesn't make the reader an expert, it's referring to the expert who wrote the paper.
Continue their careers in Virology and Epidemiology thus helping prevent future pandemics, hopefully…
https://risweb.st-andrews.ac.uk/por...ik(8f3ce432-59c0-45c0-ac90-bf2c808349ad).html
Dr Muge Cevik is a clinical lecturer in infectious diseases and medical virology. Her research interests focus on HIV, tuberculosis, viral hepatitis, emerging infections and tropical infections in LMICs.
During COVID-19 pandemic, alongside working on the front lines of the response, she provides scientific input to the Chief Medical Officer for Scotland on COVID-19 and serves as a member of NERVTAG (New and Emerging Respiratory Virus Threats Advisory Group) - an expert committee of the UK Department of Health.
https://www.researchgate.net/profile/Harry-Moultrie
Dr Harry Moultrie, senior medical epidemiologist in the Centre for Tuberculosis at the National Institute for Communicable Diseases (NICD)
I'm not taking sides. Not criticising anyone on here sorry if it came across that way. Just that there is so much info out there on the internet on every aspect of COVID from transmission to economics it's hard to sift out the bias in some of them. So easy to see how even the crackpot theories can find an echo chamber on the www.

It is the opposite of you and same as djp82 for me…. Loads of people I know have had it in last 2 or 3 weeks…. Ages 16 to 60s, office workers, manual workers, students, carers, public transport users, non PT users, no pattern at all. I would say that the last 2 or 3 weeks alone the number of people that I know testing positive matches the number I knew doing so for the entire period since testing was available.I'm the opposite - everyone seemed to have it either last autumn or in July/August, but no one recently.
Out of interest, are the people you've heard about more recent emergees? Those without much natural exposure from previous waves e.g. white collar homeworkers?
With a week or two’s more data in the bank we may well do what you suggest. Proper vaccine passports would probably also help minimal/no restrictions but there seems to be a real lack of political will for those.I just don't see why two years in with 50% of the country triple vaxxed and access to LFT testing we need to restrict living and further kill industry. People who are triple vaxxed are being Mis sold and should be allowed to do what they like in my opinion and if you test daily for work like i and many do and am also triple vaxxed it just seems nutsv
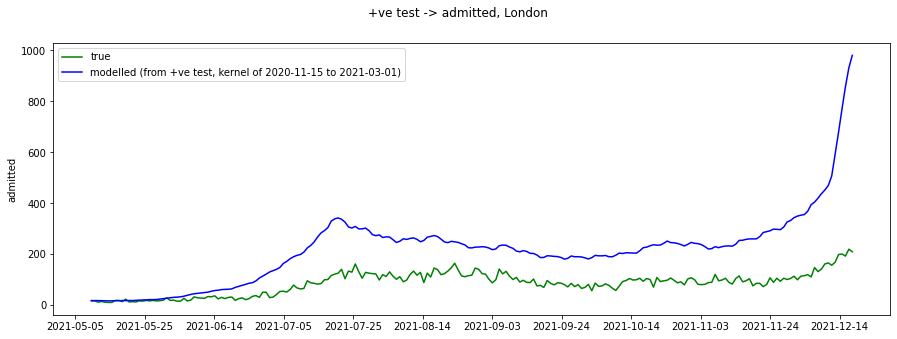
Looks like it actually shows some correlation…. The question now is whether the admissions are for COVID related illness or merely incidental. In many ways overall hospital admissions (ignoring COVID) versus a pre COVID 5 year average might be a good metric to use here to ascertain where we are.London data is showing the link between cases and hospitalisation isn't being re-established
Then you risk medical/care staff giving the virus to more vulnerable people in their place of work.If it's conclusively mild, and wiping out Delta too, then surely you just stop all isolating and also stop all testing except for severe cases (where a diagnosis can inform treatment choices)?
Back to lots of tossing I’d imagine…. Except Gutterboy…. He’ll be at Bramall Lane!COVID has created a whole industry of experts on subjects from hospital admissions, vaccine efficacy to "nudge theory." What will all these people do when the pandemic is over.
")
Then you risk medical/care staff giving the virus to more vulnerable people in their place of work.
Good point…. Though it will take a fair amount more data to prove that and we may have another less mild strain by then (that we’ve failed to identify early due to the cut in testing).If it's conclusiVely mild, does it matter?
Looks like it actually shows some correlation…. The question now is whether the admissions are for COVID related illness or merely incidental. In many ways overall hospital admissions (ignoring COVID) versus a pre COVID 5 year average might be a good metric to use here to ascertain where we are.
I don’t get how that would work? Would probably need the employer to confirm that is the case and is any employer going to do that to a member of staff? Sounds like a headline politic that one.